
In November 2025, my colleagues on the University of Michigan Faculty Senate voted decisively—67% yes, 15% no, with 18% abstaining—to urge the university’s medical school to resume providing cross-sex hormones, surgeries, and puberty blockers for patients under 19 years old. This non-binding resolution came months after our academic medical center paused these interventions in August 2025, citing a federal subpoena from the Trump administration’s Department of Justice as part of a broader investigation into pediatric “gender-affirming care.”
As a cardiologist, professor, and longtime Michigan resident, I was not surprised by the lopsided vote. Faculty senates at elite public universities often lean toward progressive positions on social issues. Still, I am deeply concerned. This recommendation places our institution at odds not only with emerging international scientific consensus but also with broader public sentiment—and, crucially, with the precautionary approach now adopted by health authorities in several European nations, as well as our own.
Michigan Medicine’s pause on “gender-affirming care” for minors was prudent, not only scientifically but legally. The DOJ probe reflects growing scrutiny of practices once promoted as unequivocally beneficial. While major U.S. medical organizations continue to endorse “gender-affirming care” for minors, including puberty blockers and cross-sex hormones, the evidence base for these interventions in children and adolescents is increasingly recognized as weak.
The landmark Cass Review, commissioned by England’s National Health Service and published in 2024, systematically examined the research on pediatric gender medicine. Led by respected pediatrician Dr. Hilary Cass, it concluded that the field is “built on shaky foundations.” The review found most studies backing “gender-affirming care” to be of low quality, with insufficient long-term data on outcomes like mental health improvement, rates of detransition, or risks such as bone density loss, infertility, and potential cancer links. As a result, England restricted puberty blockers and hormones for minors to clinical trials only.
This caution has been echoed here in the U.S. In November 2025, the same month as our faculty vote, the U.S. Department of Health and Human Services (HHS) released the peer-reviewed final version of its comprehensive report, “Treatment for Pediatric Gender Dysphoria: Review of Evidence and Best Practices.” This umbrella-review of existing systematic reviews found very low-certainty evidence for benefits of hormonal and surgical interventions, while highlighting significant, often irreversible risks. The report emphasizes therapy as the most supported approach and aligns with international findings that most gender-distressed youth resolve their dysphoria naturally post-puberty when underlying issues are addressed therapeutically.
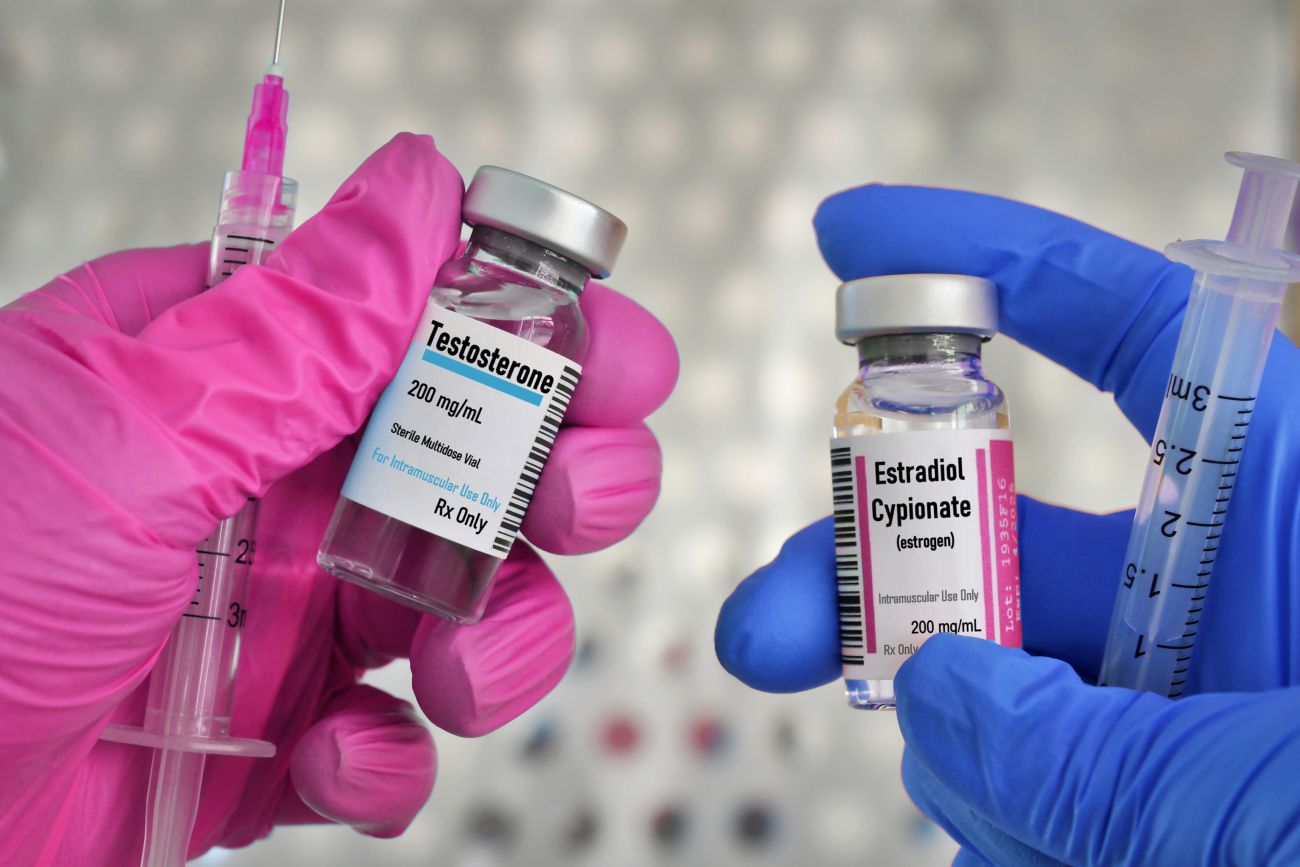
As a cardiologist, I am particularly alarmed by the cardiovascular risks these interventions pose to developing young hearts. Cross-sex hormones, such as estrogen in biological males or testosterone in biological females, are known to alter lipid profiles , increase blood clotting, and elevate the risk of thromboembolic events, stroke, myocardial infarction (heart attack), and hypertension. Multiple studies and reviews have documented these dangers: estrogen therapy may raise the likelihood of venous thromboembolism and ischemic events, while testosterone can worsen blood cholesterol and promote abnormal thickening of the heart muscle (cardiac hypertrophy). In adolescents, whose cardiovascular systems are still maturing, these effects could compound over a lifetime, potentially leading to premature heart disease—the leading cause of death worldwide.
These risks could potentially make sense if we had strong evidence of benefits over alternative approaches. But this evidence is lacking.
Public opinion in the United States adds another layer of disconnect. While polls vary in wording, a consistent pattern emerges: Americans are uneasy about medical interventions for minors. A 2023 Washington Post-KFF survey found 68% opposing puberty blockers for children ages 10-14 and 58% against hormones for minors ages 15-17. The population of Michigan, a classic purple state bellwether, likely have similar views to the nation.
The University of Michigan faculty’s push to resume care ignores these developments. It also overlooks controversies within influential guidelines, such as those from the World Professional Association for Transgender Health (WPATH). Leaked internal documents in 2024 revealed WPATH members acknowledging that many young patients cannot fully consent to the irreversible effects of “gender-affirming care” like sterility or sexual dysfunction. These files highlighted ethical lapses and a lack of rigorous evidence, further eroding confidence in the “affirmation-only” model.
At a taxpayer-funded public university like ours, especially one in a purple state, faculty governance should reflect not just internal ideologies but responsibility to scientific evidence and the communities we serve. Michigan voters and families deserve assurance that the doctors who serve them at their public medical center do no harm and respect their views.
That doesn’t mean we can’t or shouldn’t treat gender dysphoria. Indeed, we should, but we should do so via therapy, rather than permanently altering our pediatric patients’ bodies and crossing our fingers that they don’t experience life-threatening side effects.
There’s another hard truth that the Faculty Senate members—many of whom are not doctors and are unaffiliated with the medical school—presumably did not consider: people no longer automatically trust doctors or academic medicine the way they once did. Years of overreach, mixed messaging, and insistence on contested practices have left deep scars. When elite institutions charge ahead on weak evidence—especially on something as irreversible as medicalizing children’s gender distress—it confirms every suspicion that we’re more captured by ideology than we are committed to science.
Only humility will allow us to rebuild that shattered trust. Anything less, and we’ll keep hemorrhaging the one thing medicine can’t function without: the public’s confidence.